Post-Concussion Syndrome & TBI:
Symptoms, Causes & Recovery
Traumatic brain injury is one of the most misunderstood and under-treated conditions in medicine. Millions of people live with chronic symptoms - fatigue, brain fog, depression, anxiety - without ever connecting them to a head injury that may have happened years or even decades ago. This guide explains what TBI does to the brain, why standard treatment often falls short, and what newer protocols are revealing about recovery.
A New Approach to Traumatic Brain Injury

Dr. Mark Gordon is a neuroendocrinologist and the founder of the Millennium Health Network. Over the past two decades, he has pioneered a fundamentally different approach to treating traumatic brain injury - one focused on the hormonal and inflammatory damage that persists long after the initial trauma.
Dr. Gordon's work began with military veterans suffering from blast injuries and concussions who were not responding to conventional treatments. His research revealed that TBI frequently damages the pituitary gland and triggers a cascade of chronic neuroinflammation - problems that standard neurological evaluations simply do not test for.
His findings led to the development of the Millennium TBI Protocol, which uses advanced hormonal and inflammatory lab panels to identify the specific disruptions caused by brain injury, then applies targeted hormone replacement, nutraceuticals, and peptide therapies to restore function. This protocol has been used successfully in thousands of patients - veterans, athletes, accident survivors, and others living with the long-term effects of head trauma.
The Millennium TBI Protocol
A systematic approach to identifying and treating the hidden damage of brain injury
The Millennium Protocol differs from conventional TBI care in one critical way: it treats brain injury as a hormonal and metabolic condition, not just a structural one. While standard neurology focuses on the physical damage visible on imaging, the Millennium approach targets the biochemical disruptions that imaging cannot detect - but that drive the majority of chronic symptoms.
Extended hormonal and inflammatory testing far beyond what standard evaluations include: total and free testosterone, IGF-1 (growth hormone marker), full thyroid panel, cortisol, DHEA-S, estradiol, pregnenolone, progesterone, inflammatory markers (CRP, homocysteine, ESR), and more.
When lab work reveals hormonal deficiencies caused by pituitary damage, the protocol replaces those specific hormones to restore them to optimal levels. This is not generalized HRT - it is targeted based on each patient's individual lab results.
Chronic neuroinflammation after TBI is addressed through specific nutraceuticals, anti-inflammatory protocols, and in some cases peptide therapy. Reducing inflammation is critical for allowing the brain's hormonal signaling to normalize.
Patients are monitored with follow-up lab work at regular intervals. Treatment is adjusted based on objective data and symptom response. Most patients report significant improvement within 8-12 weeks of starting treatment.
What Is Traumatic Brain Injury?
A traumatic brain injury occurs when an external force disrupts the normal function of the brain. This can result from a direct blow to the head, a violent jolt or shaking of the body, or a blast wave from an explosion. TBI ranges from mild concussions to severe injuries that cause prolonged unconsciousness or amnesia.
What makes TBI particularly difficult is that the initial injury is only the beginning. The primary trauma sets off a chain of secondary biological processes - inflammation, oxidative stress, hormonal disruption, and excitotoxicity - that can continue causing damage for weeks, months, or years after the event. Many people who "recover" from the initial injury continue to experience symptoms because these secondary processes were never identified or treated.
It is also worth noting that TBI does not require a loss of consciousness. You do not need to have been "knocked out" to have sustained a brain injury. Repeated sub-concussive impacts - the kind common in contact sports, military training, and certain occupations - can produce cumulative damage that mirrors more severe single injuries.
Prevalence of TBI
Traumatic brain injury is far more common than most people realize. It is sometimes called a "silent epidemic" because many cases go undiagnosed or are attributed to other conditions like depression, PTSD, or chronic fatigue syndrome.
The leading causes of TBI include falls (especially in older adults and children), motor vehicle accidents, sports injuries (football, soccer, boxing, hockey, martial arts), military blast exposure, and assault. Veterans and athletes are particularly high-risk populations, but TBI affects people across all demographics and age groups.
TBI Severity Classification
Traumatic brain injuries are classified by severity using the Glasgow Coma Scale (GCS), loss of consciousness duration, and post-traumatic amnesia. Understanding severity helps guide initial treatment, but it does not predict long-term outcomes - even "mild" TBI can produce severe chronic symptoms.
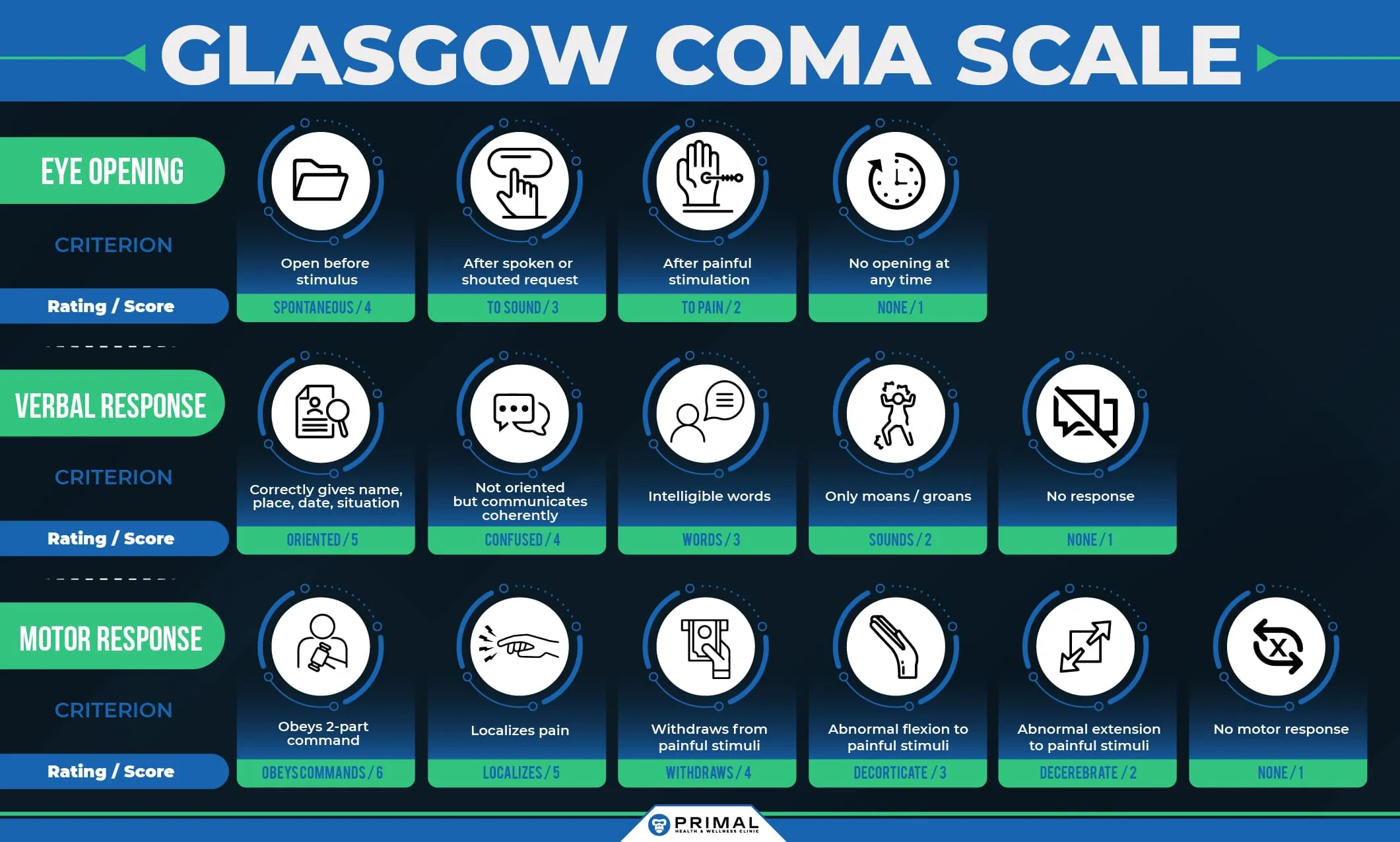
GCS score 13-15. Loss of consciousness less than 30 minutes (or none at all). Post-traumatic amnesia less than 24 hours. Accounts for approximately 75-80% of all TBI cases. Despite the label 'mild,' symptoms can persist for months or years in 15-30% of patients - a condition known as post-concussion syndrome.
GCS score 9-12. Loss of consciousness between 30 minutes and 24 hours. Post-traumatic amnesia between 1 and 7 days. Often involves structural damage visible on CT or MRI. Recovery is variable and often requires rehabilitation.
GCS score 3-8. Loss of consciousness greater than 24 hours. Post-traumatic amnesia greater than 7 days. Often life-threatening and may require surgery. Long-term cognitive, physical, and behavioral impairments are common. Even with rehabilitation, many patients experience permanent changes.
What Causes the Chronic Symptoms of TBI?
Most people assume that TBI symptoms come directly from damaged brain tissue. While structural damage plays a role in severe cases, the majority of chronic, persistent symptoms are driven by two mechanisms that conventional medicine often overlooks:
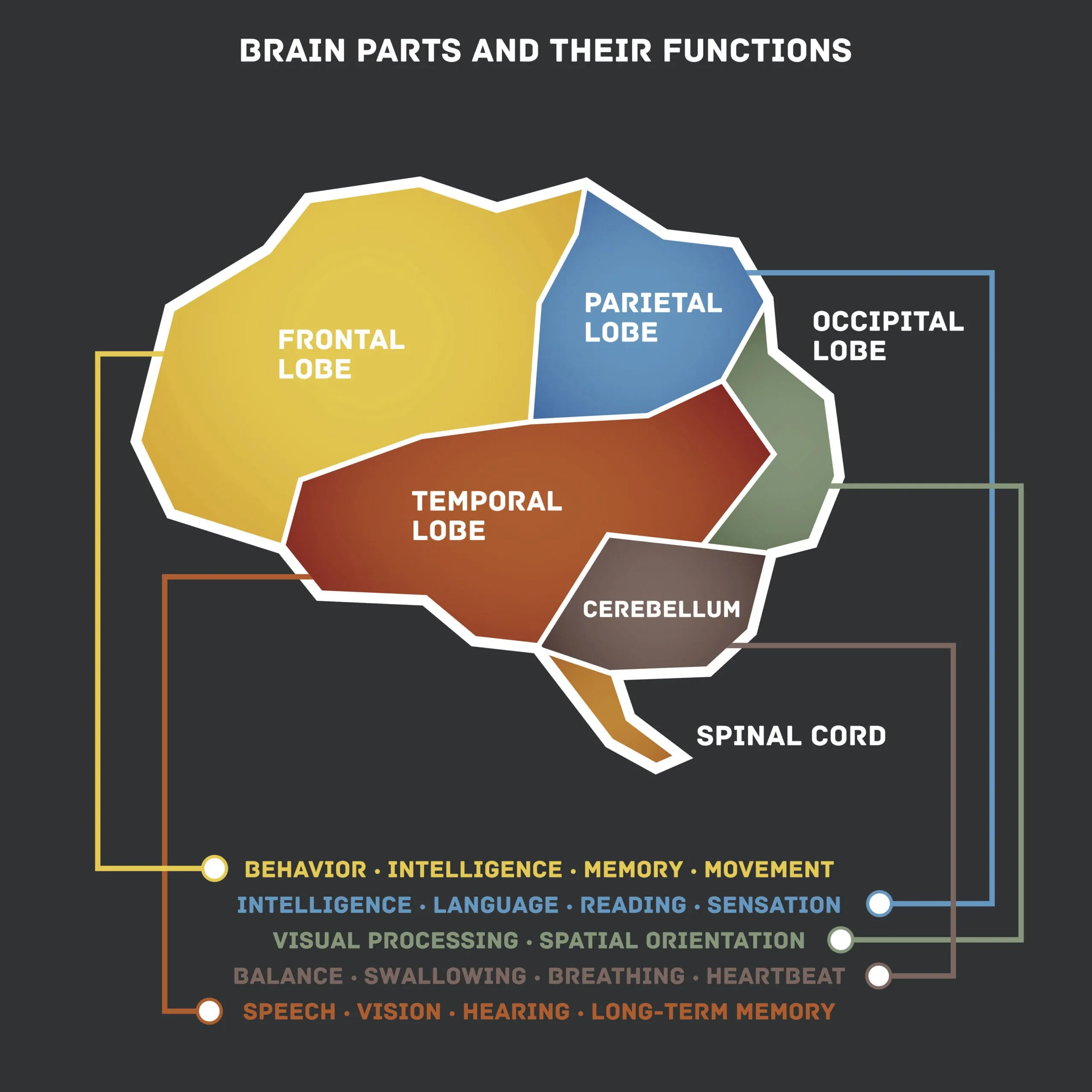
Pituitary Gland Damage
The pituitary gland sits at the base of the brain, connected to the hypothalamus by a thin stalk. Its position makes it exceptionally vulnerable to the shearing forces generated during head trauma. Even mild concussions can damage the pituitary or its blood supply.
When the pituitary is damaged, it fails to produce adequate levels of the hormones it normally regulates - including growth hormone, testosterone, thyroid hormones, cortisol, and others. When these deficiencies stem from pituitary damage following head trauma, the resulting condition is known as post-traumatic hypopituitarism - one of the most commonly overlooked consequences of a brain injury. Hypopituitarism produces many of the symptoms commonly attributed to the injury itself: fatigue, cognitive impairment, depression, weight gain, loss of motivation, and sleep disruption.
Chronic Neuroinflammation
Brain injury activates the brain's immune cells (microglia), which produce inflammatory molecules to respond to the damage. In a healthy recovery, this inflammation resolves within days to weeks. But in many TBI patients, the microglia remain activated indefinitely, producing chronic low-grade neuroinflammation.
This persistent inflammation damages neurons, disrupts neurotransmitter production, impairs the blood-brain barrier, and interferes with hormonal signaling. It is a key reason why symptoms can emerge or worsen months to years after the original injury - the inflammatory process is ongoing even when the initial trauma has long since healed.
The critical insight is that both of these mechanisms are testable and treatable. Hormonal deficiencies show up on blood work. Inflammatory markers can be measured. And when treatment addresses these root causes, many patients experience dramatic improvement in symptoms they have lived with for years.
Common Symptoms of TBI
TBI symptoms are wide-ranging because the hormonal and inflammatory disruptions affect nearly every system in the body. Many of these symptoms overlap with other conditions, which is why TBI-related hormonal dysfunction is so frequently missed.
If you are experiencing a cluster of these symptoms - especially following a known head injury, blast exposure, or history of contact sports - a comprehensive hormonal and inflammatory evaluation may reveal treatable causes that have been overlooked.
Traditional Approach vs. Millennium Protocol
The traditional medical approach to TBI and the Millennium Protocol approach represent fundamentally different philosophies about what causes chronic symptoms and how to treat them.
| Traditional Approach | Millennium Protocol | |
|---|---|---|
| Focus | Structural brain damage | Hormonal and inflammatory disruption |
| Primary tools | Imaging (CT, MRI) | Advanced blood panels (50+ markers) |
| Symptom view | Direct result of brain damage | Often caused by treatable deficiencies |
| Depression treatment | Antidepressants (SSRIs) | Address hormonal root cause first |
| Fatigue treatment | Stimulants, sleep hygiene counseling | Restore growth hormone, thyroid, testosterone |
| Timeline | Wait and see, symptoms may resolve | Active intervention, measurable results in 8-12 weeks |
| Old injuries | Limited options, symptom management | Same protocol regardless of injury age |
Additional Resources
Learning about traumatic brain injury is the first step toward understanding your symptoms and exploring treatment options. The following resources provide additional information about the Millennium TBI Protocol and the research behind it.
The official resource of the Millennium Health Network. Includes information about Dr. Mark Gordon's research, the TBI protocol, provider directory, and patient resources.
Learn about our TBI evaluation and treatment services. Dr. Strand is a member of the Millennium TBI Network, West Point graduate, and Army combat veteran.
Think Your Symptoms Might Be TBI-Related?
If you have a history of head injury, blast exposure, or contact sports and are living with chronic symptoms, a comprehensive hormonal and inflammatory evaluation can reveal whether treatable disruptions are driving your condition.